Several countries finances nursing services within the framework of the so-called Nursing Care Insurance – from an independent account – in order to monitor nursing costs, the effective utilization of financial sources, and lastly, for the servicing of the treatment of patients requiring care within the framework of an insurance scheme. Germany, the Netherlands, the UK, the USA, Israel manages the costs of the monitored services of the service providers, while e.g. Austria provides an amount designated for the purchase of a specific service for the patient. The budget is regulated by law in all countries. In Hungary, we have made the first step on the way to establishing nursing insurance by the establishment of professional home nursing services and realizing their independent financing. The Hungarian system is equivalent to the German nursing insurance system, the establishment of a Hungarian nursing care insurance system is the most easily executable using the German model.
We highly recommend to develop funding codes, and to carry out code development/code maintenance/review for professionals (especially nursing) – similar to medical practice as in existing areas which could be examples (physiotherapy, dietotherapy). However, the development of professional protocols will be essential which should be interpreted equally throughout the caring system. Based on the good evidence based practice, it is necessary to develop nursing protocols, without this, patient safety cannot be increased, the incidence of nosocomial infections cannot be reduced, and the negative consequences of unreasonable and/or old and outdated equipment and/or old and outdated practices and/or even the negative consequences of interventions within the institution with significant differences cannot be dismantled. Extensive collaboration, good methodology, foreign language knowledge and literature researches are essential to the development process, beyond the knowledge of national practices. The development work carried out so far in this field with extensive cooperation in respect of the Textbook of Nursing Science can serve as a good example. This is also essential to provide the appropriate professional background for skill/simulation practices.
For the sake of the professional representation of the nursing profession, the establishment of an independent Nursing Department within the Ministry of Human Capacities and the improvement of the apparatus, with special regard to the national- and international representations of the several hundreds of thousands of professionals including tens of thousands of nurses, to the departmental control covering professional education, to the reformation of the mandatory continuous developmental system and the importance of the professional’s certification system.
Establishment of the Government Chief Nursing Officer (CNO) position on state level with the relevant scope of practice and infrastructure to support and influence professional political decisions. The re-establishment of the national professional monitoring system, for the inspection of the external and internal quality management system’s operation.
Opposite the former systems, the current system of the Hungarian vocational nurse education – in which a general nursing- and health care assistant qualification, a practicing nurse qualification following the 12th semester, and finally a nurse qualification can be acquired within the framework of the vocational high school education – does not fulfill the minimum requirements defined in the relevant 2005/36 EU directive (European Committee, 2005/36/EK order), which are obligatory for Hungary as well (Figure 7). According to the 2005/36/EK directive, the nurse education can be initiated from the 10th grade, it may be continued in a day work schedule in the form of a minimum 4600-hour and 3 year education. The Hungarian vocational nurse education – deviating from the directive – begins from 9th class (cumulative and offset), it may be continued in full- and part-timework schedules as well, in which the number of hours can be 1527, while in the case of full time education, the number of hours can be between 3214 (two-tier education) and 3639 hours (three-tier education) (in case if we incorporate the relevant hours of the vocational high school education, although the EU directive only allows incorporation from an equivalent level of education).
In consequence of the above, the following crucial situation has emerged: regarding the Hungarian vocational nurse qualification, the National Healthcare Service Center is legally unable to issue compliance to the minimal requirements of the 2005/36/EK Union policy following 2012, thereby the official certificate for EU conformity, also, without the radical modification of the system, an infringement procedure can be initiated against our country, and our nurse education may be excluded from the automatically certified qualification based on community law.
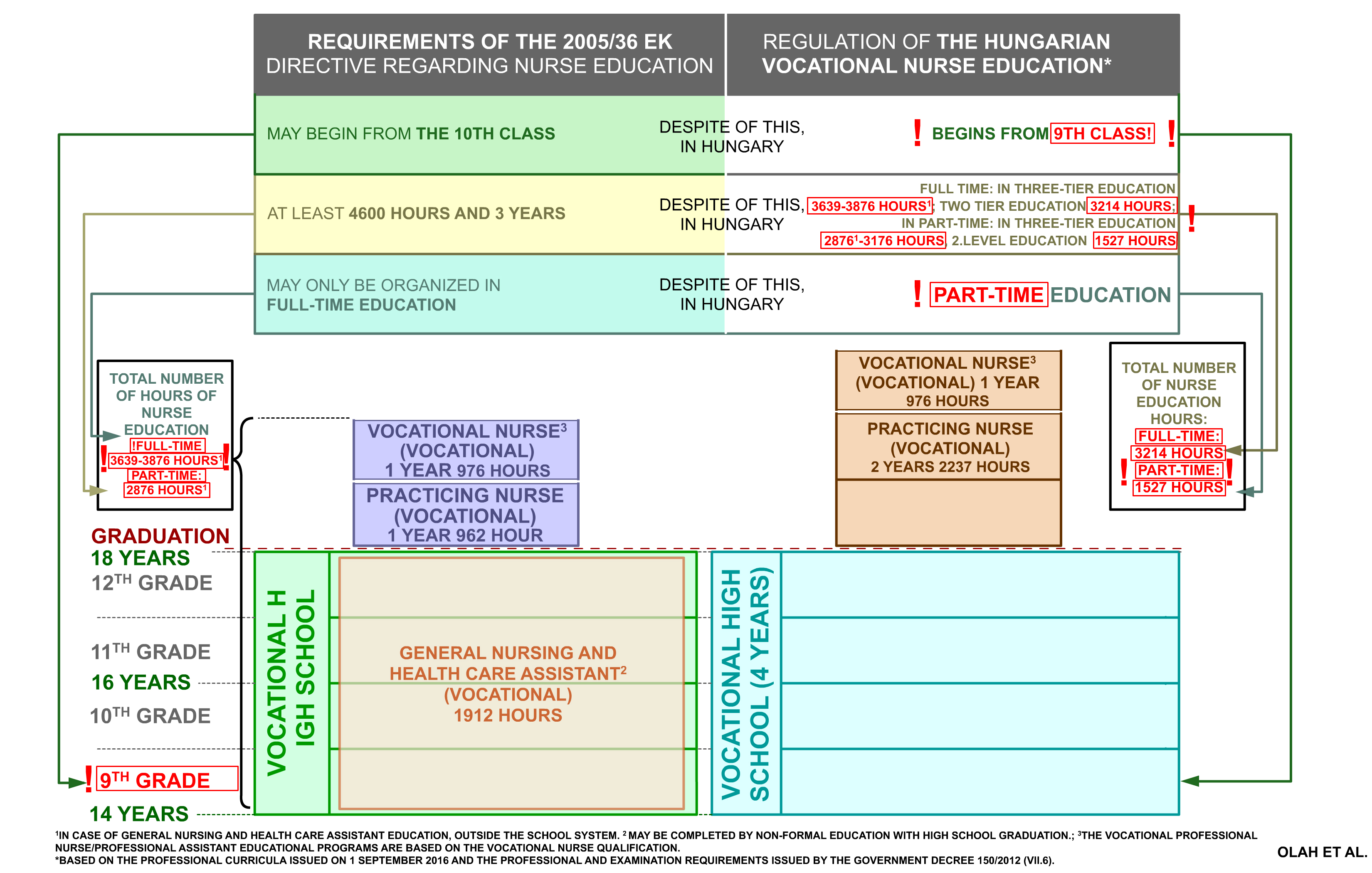
Figure 7. Framework for regulating vocational nursing education in Hungary compared to the requirements of EU Directive 2005/36 on nursing education
With the introduction of the vocational high school system, the Ministry of National Economy determined the maximum number of hours of the 4+1 year vocational high school professional education and the professional qualification-augmentation (with which the number of hours required by the 2005/36/EK directive cannot be provided regarding nurse education). Instead of the 4600-hour education prescribed by the EU directive, and adapting to the framework determined by the NGM, the total number of hours in case of a three-tier education is (general nursing- and health care assistant, 1 year practicing nurse, 1 year nurse): 3851 hours in full-time work schedule, with school-system general nursing and health care assistant education, in case of nursing- and health care assistant non-formal education, it is 3639 hours, in part-time work schedule, in case of general nursing- and health care assistant non-formal education is 2876 hours. In case of a two-tier system (2 year practicing nurse, 1 year nurse), in a full-time work schedule, it is 3214 hours, in a part-time work schedule, it is 1527 hours. The determined number of hours is professionally unsuitable, since there is not enough number of hours for the deepening of certain curricular contents within the nursing education compared to the practicing nurse, and in case of the latter, to the general nursing- and health care assistant education. For example, anatomy- and physiology education is no longer available in the practicing nurse- and nurse educational programs, i.e. only the 9th grade general nursing- and health care assistant education provides anatomy-physiology education, while these are crucial for both educational programs based on them due to the wider scope of practice of the practicing nurse- and nurse educational programs.
The latter is also rendered impossible by the fact that the qualification of the subject teachers is insufficient (e.g. the education of clinical practice and pharmacology can be conducted by Bachelor nurses and health care vocational teachers as well), while according to the professional and exam requirements, the vocational nurse receives an independent scope of practice for prescription and ordering infusion therapy (compared to the practicing nurse education, with 17 further hours of pharmacology education, and without anatomy/physiology education within the practicing nurse/nurse educational programs). These facts also show that the scope of practice circle determined by the professional and exam requirements and the Curriculum-designated competencies to be developed contain several elements which the student cannot be prepared for (e.g. prescription, arterial puncture). Further anomalies of the education framework in their case: they study internal medicine, surgery, pediatrics subjects in the first school year, while studying the anatomy and pharmacology at the same time in second year, and basic therapeutic knowledges in the second semester. These students need to learn more than 20 topics in the first school year, which is neither professional nor pedagogical. While students come out with lower basic skills, many children find it very hard to share their attention on so many topics. Many find it difficult to read and study a foreign language (English/German/Latin). Because of all this, the drop-out rate is high in the first half of the year, so the scholarship system cannot fulfill its motivating role.
A further problem is that while earlier the entire nurse education could be completed in a non-formal model, currently only the general nursing- and health care assistant and several professional assistant educational programs can be completed in a non-formal model, which is not compliant to the requirements determined in the 36/2005 EK EU directive. The problems with the non-formal system are the following: they can be organized within the framework of individual preparation, grouping and distance education, thus it can be completed without manual competency examination and demonstration, the examination of practices are not- or only demonstrated in writing, which is a severe professional problem. Its number of hours is significantly lower compared to the school system, any legal person can initiate such an education following accreditation, and accreditation is examined by the organization of the Hungarian Chamber of Commerce and Industry with territorial competency. The institution is not obligated to possess any king of equipment, the accreditation can be realized by the presentation of a framework agreement with the inclusion of professionals requested by the Hungarian Chamber of Commerce and Industry. While in the school system, the number of hours is determined by programs and subjects, in the non-formal educational system, every number of hours is regulated within a significantly broader framework. The curriculum-content, technical literature background and teachers of the formal educational programs are all regulated. The formal educational programs possess central framework curriculum, while the non-formal educational programs only need to adhere to the regulations determined by the Vocational exam requirements (SZVK), and only a fraction of the module content (e.g.: task profiles) are highlighted. We suggest the verification of the sectoral professional educational programs and determining, which given vocational education forms cannot be organized in case of adult education in point 7. of the Vocational exam Requirements. Aside from that, it is necessary to discontinue the non-formal educational model in case of the general nursing- and health care assistant education as well.
The Ministry of National Economy has determined the number of modules and programs as well as their characteristics within the formal educational programs. Certain worthy fields cannot occur as independent programs, only as subjects within a program, e.g. anatomy-physiology is only a subject within a program, which constitutes as one program together with further 4 subjects (e.g. first aid), which is evaluated with a common grade. Aside from that, the classroom and demonstrational practices were eliminated, which – along with theoretical education – is crucial for the acquisition of certain interventions and cannot be supplemented by hospital practice.
The status of the sectoral professional education is further worsened by the fact that there is no national unified system regarding the incorporation of previous specialized professional knowledge – section (1) of par. 22 of the 2011 CLXXXVII. act –, the degree of incorporation is based on subjective evaluation as determined by the professional program, which differs by schools/educational institutions. We also have knowledge about cases where the degree of incorporation is not uniform regarding students with equivalent professional backgrounds, and there are also cases where a given incorporation is not justifiable professionally. The subjectivity available creates a possibility for vulnerability both in formal- and non-formal educational programs. Last, but not least, the degree of acceptance is not irrelevant from the point of professionalism – human resources education – either. The lack of a national unified incorporation system is a problem regarding formal educational programs, however, it is an even greater problem regarding market-based, profit-oriented teachers with- or without legal personality, where occasionally the aim could be the reduction of costs and the increase of competitiveness (shorter period of educational time compared to other, profession-based educational institutions), the unrealistic decrease of educational time by exploiting the possibility of incorporation, often disregarding professional interests. The establishment and coordination – within the framework of a suitable ministerial background institution – of a national unified system regarding the system of incorporation.
The 2011 CLXXXVII. act on professional education enabled the realization of a dual educational structure regarding health care educational programs since January 1, 2013. For the sake of a uniform theory and practice, a close cooperation between the school and the practice educational establishment is essential (obligatory documented consultations between the educational institution of theory and the organizer/performer of the internship), to which the demonstration of the nationally unified and observed program description/subjects and its provision to the organizer/performer of the practice is closely connected; it constitutes as the basis for practical education, aside from a well-constructed educational structure. This way, the acquisition of practical knowledge related to the theoretical educational subjects can be realized, as well as the development of competency, capability and manuality.
However, currently the practical placements in dual education are unregulated, making the output requirements of the vocational education very difficult. The biggest problem is that there are no proper professional and legal requirements for the number of staff with professional competence to make professional practical placements. While this is regulated in the public education system, this is missing in the practical educational institutes. It is not known, regarding to the given practical educational institute, whether there is an independent vocational lecturer; the number of students per lecturer and what specific expectations should the lecturer met in practical experiences, and in pedagogical, or professional point of view. If a mentor performs the task, the question is if the mentor does it in parallel with a daily nursing job (for example if there is a ward with 50 beds and 2 nurses, and one of them is the mentor) when does the mentor have time for students and for workflows which should be trained professionally for future nurses.
Pupils in the 11th grade are already practicing in curative wards. A permanent supervision should be provided for them because they see a naked body for the first time, who needs help in self-hygiene and defecation. They first meet with dying and dead care, for which they are not really prepared, they see bleeding and purulent skin etc. for the first time. The experience gained here greatly inhibits in many cases the successful career motivation of students.
In the case of a 2-year-long nursing assistant education after high school, according to the subjects, the practical education can not follow the theoretical education, therefore students attend practical placements without professional knowledge.
The definition of dual education is part of 108. § 1 b. Section of the National Higher Education Act. According to it, the dual education is: “the form of education for the practice based Bachelor education, in the area of information technology, agriculture, natural sciences and economic sciences and the belonging master educations, where according to the education and qualification requirements- the practical education is a full time study, its curriculum contains directives regarding the study time, study method, lectures, individual evaluation of the gained knowledge and taking part at qualified organisations within frames defined by the Dual Educational Committee”.
This way, the dual education is a form of a practice based education in Bachelor level, where the practical internships at professionally qualified employers increase the professional competence and strengthen his culture though their curricular content, structure, increased amount of practical hours spent at the employer as well by the earned work experience. As in the case of dual education, during the education the cooperating employer also formally teaches the students in a predefined way, closely fit to the curriculum of the higher education institution. With the support of this educational system a workforce leave the higher education, who is able to enter the workplace immediately, without any further financial expenditures or year’s long additional training. This means, it is a quick and effective tool in the solution of labour shortages on qualitative level.
Currently there is no dual education in the higher education in the medical-health care educational area in accordance with National Higher Education Act, however considering the practice orientation of the model, it is appropriate to analyse the integration of the health science related studies into the dual education system. Despite of the fact, that the workplaces can only functioning as dual partnerinstitutions, these are solely state financed institutions, the integration of the dual education system should be part of the national strategy, it could be essential in the labour force replacement in healthcare, because the main problem regarding the human resources is the unpredictable fluctuation, this way the resupply of professionals could be plannable. The institutional support for students, which means 65% of guaranteed minimum wage can support a livelihood in the short term beside the existing, normative-based social and performance-based bonuses.
The lack of nationally unified and obligatory, up-to-date professional textbooks with suitable professional content as well as the recommended professional material and policies is an issue closely connected to the above-mentioned problems. In order for the quickest and most simple possible realization regarding the curriculum/subjects, it is suggested and practical to provide electronic access to the curriculum, which may facilitate the provision of a unified education.
The textbook background of nursing education is appropriate to expand additionally. A good example of this is the publication of the electronic textbook “Nursing Science” in 2012, which was a true niche to the literature on nursing education in Hungary, since it is an innovation in health education and practice in order to promote the introduction of international practice based on modern evidences.
It is known that the number of general education subjects was decreased (in case of our department, chemistry, physics and geography may be eligible for education above the scarce number of hours of the complex natural science subject), therefore, one general education subject remains by sector; in case of health care, it is biology. Aside from that, contrary to high schools, only one foreign language subject is possible, while a language exam will become a mandatory entrance requirement in academics by 2020. These factors complicate not only the flexible compatibility to future challenges, but the application for higher education as well. Since only biology possesses a suitable number of hours, the student – regarding the subjects mentioned above – will not necessarily acquire an opportunity for a high school/secondary school leaving exam on an intermediate/advanced level, complicating his/her continuous development. Due to the 2017 legislative amendment, the vocational high school education provides an additional vocational qualification as well, although this is optional for the students and not mandatory. This may result in a problem for two reasons: first, it cannot fulfill its role regarding our sector, (“promotes transition to higher-level educational programs, provides the conditions for development, studying and re-educating, it conforms to the changes and the continuous developments in a flexible manner”) and it cannot provide a suitable number of young workforce with utilizable professional qualification, second, the student can also end up in a difficult situation, since he/she may qualify in the professional high school without professional qualification and without the opportunity to apply for academic studies. All this, while in Hungary, it takes 1912 hours in 4 years set to the age of 18 years and a high school/secondary school leaving exam for the general nursing- and health care assistants to acquire the same scope of practice as the nurse assistants receive internationally (e.g. England, USA) with 150-200 hours in 1-2 months – even by theoretical education conducted via e-learning.
According to a 2017 amendment, the vocational exam of the general nursing and health care assistant education has been moved to the February/March period (despite the opposition of the professional experts and the lector). This is a problem due to the fact that the framework curriculum determines the annual number of hours per week, and the high school/secondary school leaving exam cannot be initiated without the acquirement of the knowledge determined in the framework curriculum, i.e. the student is obligated to complete the given curriculum in 3,5 years instead of 4. Filling out the remaining time frame – generated by the preliminary qualification exam – is not regulated by law nor by the framework curriculum, therefore the institute decides on it of its own competence and the number of utilizable hours regarding the professional education and the exam decreases, while the minimal number of hours prescribed by the 2005/36/EK directive was not achievable already. By the recommendations of the Ministry of National Economy and the Adult Education Regulation Department, the rules of the high school/secondary school leaving exam will change as well. According to the change, the sectoral professional written school-leaving exam (in which the level of satisfactory completion is 25%) will be incorporated as grade of five - regardless of the achieved grade - will replace the auxiliary professional qualification’s professional closing exam (in which the level of satisfactory completion is 51%), while only covering 60% of it.
Unfortunately, the competence system within the health care sector was discontinued, thus, the suitability of applied candidates is not assessed from a health, psychological or physical point of view before the start of the education programme. The occupational health service usually focuses on the health status of students starting practical placements, or on those who obtained a degree and are already on the labor market. The nursing profession, working with individuals puts serious physical and mental stress on the person. For example: the nurse is required to apply sufficient force during the mobilization of the patients, which may result in serious complications among employees above 4 dioptres; they also required enduring the sight of blood. The health care profession is also not recommended for individuals with certain infectious- or skin diseases or allergies, as the worker’s- or the patient’s health might become of risk. The nurse needs to communicate with individuals and help them, therefore if he/she cannot suitably treat the clients entrusted on him/her due to his/her communication- or movement deficiencies, he/she cannot receive work. A health care worker might enter the workforce, who is mentally unsuitable to perform tasks, however, a person may acquire a qualification with physical/mental deficiencies. For these reasons, the restoration of the competence system in the health care sector is justified.
In order to educate professionals with suitable qualification in the educational programs within the health care sector, it is exceedingly important to have an admission procedure with a written competitive exam (e.g. biology) and an oral interview following their registration into the professional educational system, in order to eliminate unsuitable students before the initiation of the education, based on their professional knowledge or even their personality traits. Students unsuitable for the practice of the profession can severely complicate the realization of the theoretical and practical education, the transferring of knowledge with their negative attitude, their disruptive effect is perceivable regarding the students suitable for the practice of the profession as well. The stress is realized even on a national economic level. A portion of these students – in a certain section of the educational process – often leave education, the invested normative support is practically wasted, as well as the invested energy and costs. The admission procedure system worked in the educational structure preceding the vocational education, which was unfortunately abolished later.
Unfortunately, the vocational health care educational system does not directly fit to the Hungarian Qualifications Framework established according to the European Qualifications Framework; remedying this problem is crucial.
We will discuss later, but it is also important to briefly mention here the problems of practical training when reviewing the training as a whole. The basic problem is the lack of trainers and lecturers in the institutions, lack of mentors and the fact that they are unable to deal with the students or they are absent. In addition, there is a problem with practical trainings according to vocational trainings, with vocational qualification, but without higher education degree in educational qualification practical lecturers or trainers cannot hold a practical lecture, which may lead to further serious problems with the education due to the lack of professionals (see in II.11.4).
There is still a sufficient opportunity to support the fields of professions as state funded education, where is a significant demand on workforce. Although it is also important, not to support educations, where is no significant lack on workforce. Unfortunately the health masseur education became as state funded education, which is not justified. At the same time, there is a misuse regarding the state funding in the fields of professions, where is a significant demand on workforce. For the participants of trainings, organized by the unemployment offices the tuition fee of the training will be financed as state funding and in dual education the participant get a significant financial support. At the same time, in the case of an unsuccessful vocational examination (not even for the second try) it is not necessary to pay back the received support. Neither this, nor the unjustified support of certain trainings contributes to the shortage of professionals in the areas affected by the shortage of labor, and therefore changes to the system are needed.